Abstract
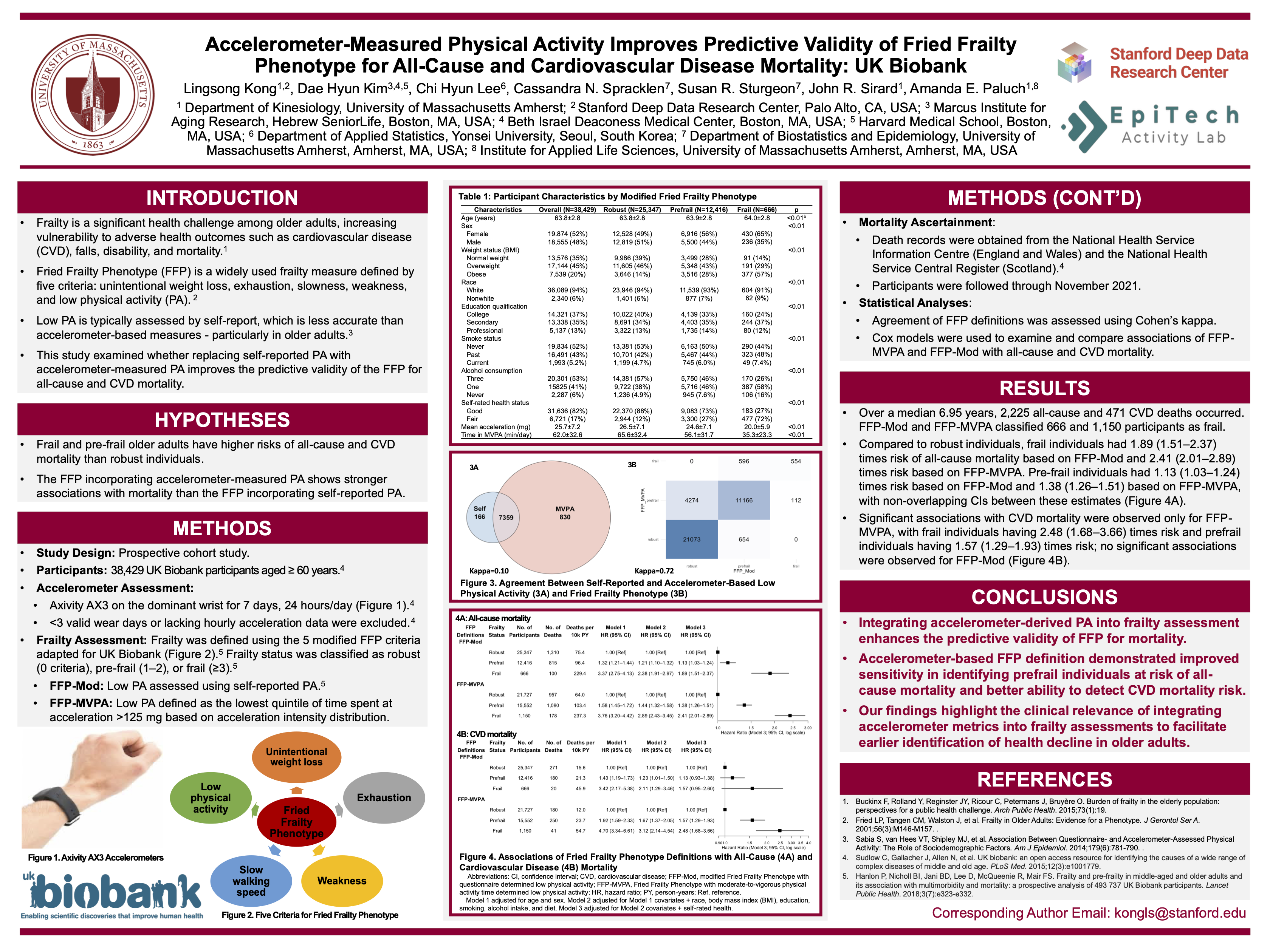
This prospective cohort study examined whether accelerometer-measured physical activity (PA) improves the predictive validity of the Fried Frailty Phenotype (FFP) for mortality compared with self-reported PA. The sample included 38,429 UK Biobank older adults (63.8±2.8 years; 48% male) with valid accelerometer and frailty data. Frailty was defined using five FFP criteria (frail ≥3; prefrail 1–2; robust 0) under two definitions: questionnaire-based FFP (FFP-Mod) and accelerometer-based FFP (FFP-MVPA), with low PA defined as the lowest quintile of moderate-to-vigorous PA. Over a median 6.95-year follow-up, 2,225 all-cause and 471 cardiovascular disease (CVD) deaths occurred. Compared with robust individuals, frail individuals had higher all-cause mortality risk under both FFP-Mod (HR 1.89, 95% CI 1.51–2.37) and FFP-MVPA (HR 2.41, 95% CI 2.01–2.89). Prefrail risk was higher for FFP-MVPA (HR 1.38, 95% CI 1.26–1.51) than FFP-Mod (HR 1.13, 95% CI 1.03–1.24). Only FFP-MVPA–defined prefrailty (HR 1.57, 95% CI 1.29–1.93) and frailty (HR 2.48, 95% CI 1.68–3.66) predicted CVD mortality. Integrating accelerometer-derived PA enhances the mortality predictive validity of FFP.