Title: Accelerometer-Measured Physical Activity Improves Predictive Validity of Fried Frailty Phenotype for All-Cause and Cardiovascular Disease Mortality: UK Biobank
Authors: Lingsong Kong, Dae Hyun Kim, Chi Hyun Lee, Cassandra N. Spracklen, Susan R. Sturgeon, John R. Sirard, Amanda E. Paluch
Abstract: Introduction: Fried Frailty Phenotype (FFP) is a widely used frailty measure defined by five criteria: unintentional weight loss, exhaustion, slowness, weakness, and low physical activity (PA). Low PA is typically assessed by self-report, which is less accurate than accelerometer-based measures. This study examined whether accelerometer-measured PA improves the predictive validity of FFP for mortality.
Hypothesis: Frail and prefrail older adults would have higher risks of all-cause and cardiovascular disease (CVD) mortality than robust individuals. FFP incorporating accelerometer-measured PA would show stronger associations with mortality than that using self-reported PA.
Methods: This prospective cohort study included 38,429 UK Biobank older adults (mean age 63.8±2.8 years; 48% male) with valid accelerometer and frailty data. Frailty status was defined by 5 FFP criteria (frail ≥3; prefrail=1–2; robust=0). Two definitions were used: FFP-Mod (questionnaire-based) and FFP-MVPA (low PA as lowest quintile of accelerometer-measured moderate-to-vigorous PA time). Cox proportional hazards models examined associations of frailty with mortality, adjusting for demographic, lifestyle, and health covariates.
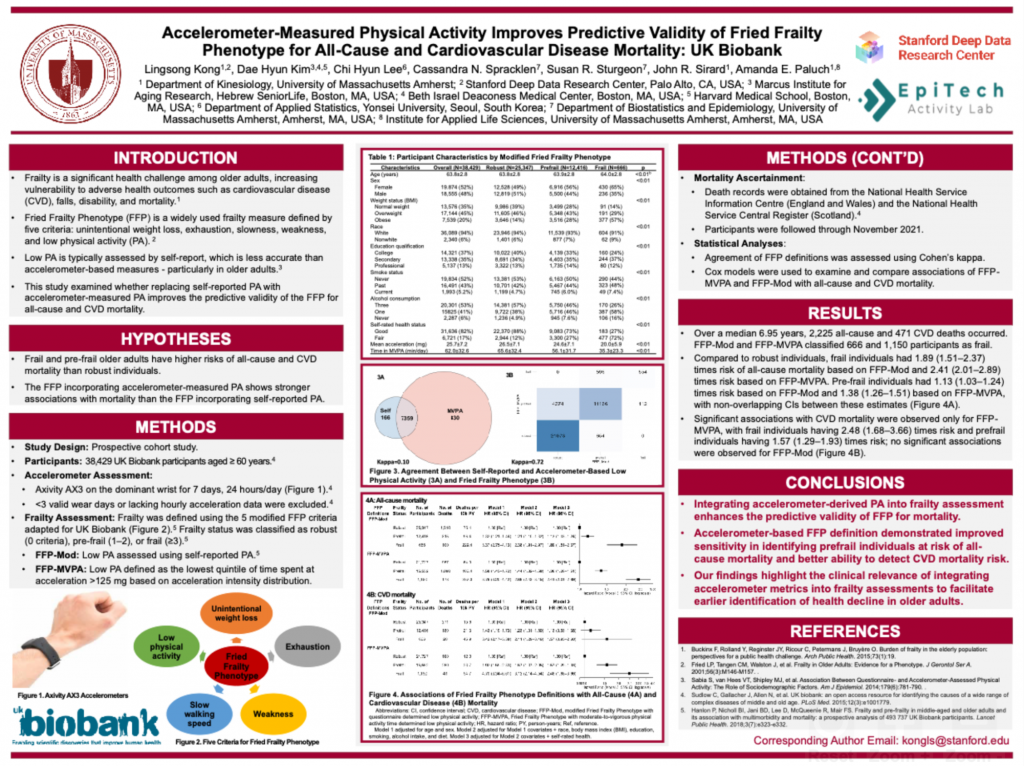
Results: Over a median 6.95-year follow-up, 2,225 all-cause and 471 CVD deaths occurred. FFP-Mod and FFP-MVPA classified 666 and 1,150 as frail. Compared to robust individuals, frail individuals had 1.89 (95% CI: 1.51–2.37) times risk of all-cause mortality based on FFP-Mod and 2.41 (2.01–2.89) times risk based on FFP-MVPA. Prefrail individuals had 1.13 (1.03–1.24) times risk based on FFP-Mod and 1.38 (1.26–1.51) based on FFP-MVPA, with non-overlapping CIs between these estimates. Significant associations with CVD mortality were observed only for FFP-MVPA, with frail individuals having 2.48 (1.68–3.66) times risk and prefrail individuals having 1.57 (1.29–1.93) times risk; no significant associations were observed for FFP-Mod (frail: 1.57, 0.95–2.60; prefrail: 1.13, 0.93–1.38).
Conclusion: Integrating accelerometer-derived PA into frailty assessment enhances the predictive validity of FFP for mortality. The accelerometer-based FFP definition demonstrated improved sensitivity in identifying prefrail individuals at risk of all-cause mortality and better ability to detect CVD mortality risk. These findings highlight the clinical relevance of integrating accelerometer metrics into frailty assessments to facilitate earlier identification of health decline in older adults.